Our opportunity to temper the torment of silent suffering

 UICC 2021")
In writing on the topic of access to essential palliative care medicines for people living with cancer, I considered speaking as a biomedical researcher or as a clinical neuropsychologist. I was even tempted to focus on regulations related to controlled medicines and health equity, based on my international policy experience. All are relevant to the issue.
However, I am sharing a fundamental, human perspective because the reality is that pain does not recognise science or policy. Suffering disregards academic degrees. Pain is the great equaliser; suffering is a mighty unifier. Pain, including pain caused by cancer, cuts across every age, gender, race, ethnicity, socio-economic and educational status. Cancer and pain can – and often do – threaten one's quality of life and very existence.
Denying palliative care medicines destroys dignity
What motivates advocating for essential palliative care medicines? I have experienced and witnessed the ravages of lack of access to palliative care and medicines for relief. Another major influence is my great-grandmother, who suffered from cancer fairly young. Then, there were few treatments for cancer, but the “gold standard” palliative care medicine (morphine) could provide pain management. Sadly, she was denied such relief. Neighbours who worked at the hospital where she spent her last days said they could hear the cries of agony from her and other women with cancer reverberating several floors up. Although cancer took their lives, unremitting pain and unconscionable suffering – because of lack of palliative care medicines – took their dignity.
Dignity and humanity are lost when people are denied palliative care medicines that can effectively treat cancer-related pain and mitigate needless suffering.
Why bother with science? Because “Pain Can Kill”
Research abounds demonstrating the multidimensional bio-psycho-social effects of pain. In “Pain Can Kill”, legendary pain researcher Dr John Liebeskind revealed how pain causes pathologic changes to the nervous system and how unmanaged pain can suppress Natural Killer (NK) immune system cells, which play an important role in fighting cancer. Dr. Liebeskind asserted that pain should not be regarded as a mere symptom but as a factor that inhibits healing and can cause tumours to spread more rapidly.
Although his research primarily used animal models, his work serves as a foundation and inspiration for my own translational research and advocacy to address the potentially lethal effects of unmanaged pain, especially among people with cancer. This and other scientific evidence support a moral imperative to effectively manage – if not eliminate – pain, as remission and life may depend on it.
Pain devastates lives and palliative care brings a touch of humanity
Pain affects every aspect of one’s life. Though pain is individual, it is not experienced alone. Bearing witness to a person’s pain affects families, communities and societies. If ineffectively managed, associated suffering leaves devastating memories. Together, we have the opportunity to profoundly touch lives by how we serve those suffering in pain.
Palliative care is a specialised, interdisciplinary service that treats the “whole person” and regains a sense of humanity. It is a human-centred, holistic approach addressing mind-body-spirit and one’s social milieu. Palliative care is not about cure but focuses on relief and comfort. Relief from cancer-related pain is an unimaginably precious gift for the suffering. Unfortunately, it is elusive to billions of people.
Collectively temper the torment and regain a sense of humanity
Since 1977, the World Health Organization (WHO) has had opioids on their List of Essential Medicines designated for pain management and recently palliative care, with morphine being the most effective and affordable. Global organisations such as the International Narcotics Control Board (INCB), the United Nations Office on Drugs and Crime (UNODC) and WHO repeatedly assert that governments must ensure adequate access and availability to internationally controlled substances (i.e. opioids) for medical and scientific purposes, especially pain and palliative care. Yet, most of the world’s population has little or no access to these medicines.
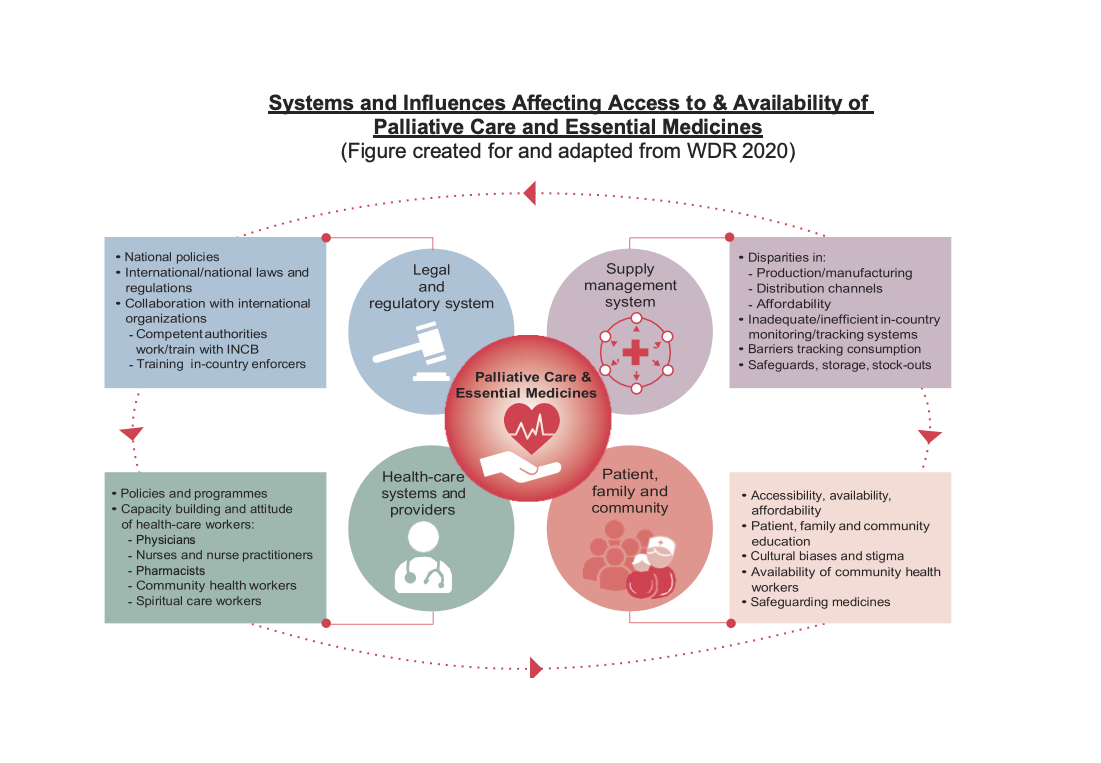
The reasons are profoundly complex and span governments, economies, communities and families, while patients lose quality of life and dignity. Thus, millions suffer in silence or scream in agony, victims of the “access abyss” that further entrenches profound disparities.
The WHO Constitution envisages “…the highest attainable standard of health as a fundamental right of every human being” while the UN Charter and Declaration of Human Rights reaffirm the dignity and worth of each human.
Denying access to palliative care medicines sends a message of unworthiness. Barriers to palliative medicines obstruct human rights. We must hear the silent screams of those who have little or no access to palliative medicines, collectively marshal our forces and take this opportunity to temper their torment.
This can only be accomplished with measurable and collective efforts to eliminate barriers, reduce disparities and improve access and availability of palliative care medicines globally. It is in that way that we may regain critical components of our humanity – dignity, respect, and quality of life, which include palliative care and relief of suffering.
Related links
Last update
Monday 05 December 2022

{kind=link}